
Use our readymade template to create this Google form. Customize it further using our form builder.
Create your intake form
- Use prebuilt template to create a HIPAA compliant online podiatry intake form
- Collect patient, demography, emergency contact details, medical history
- Collect foot-related concerns, pain level, and lifestyle impact
- Allow patients to upload their driver’s id, prescriptions for medications
- Get signatures for consent for treatment, notice of privacy practices, use of PHI
Collect responses from your patients
| Patient ID | user input |
| Patient Name | user input |
| Patient Email | user input |
| Patient Phone Number | user input |
| Marital Status | user input |
| Date of birth | user input |
| Address | user input |
| Emergency Contact Name | user input |
| Emergency Contact Phone | user input |
| Relationship | user input |
| Primary Doctor | user input |
| Location | user input |
| Date of service | user input |
| Primary Insured (subscriber) | user input |
| Relationship to Patient | user input |
| Date of Birth | user input |
| Phone number | user input |
| Subscriber Employer or Plan Sponsor | user input |
| Insurance Company | user input |
| Subscriber ID# | user input |
| Secondary Policy Holder Name | user input |
| Date of Birth | user input |
| Subscriber Employer or Plan Sponsor | user input |
| Phone number | user input |
| Insurance Company | user input |
| What are the medical issues concerning your foot, ankle and legs? | user input |
| Result of accident or work injury? | No |
| On a scale of 1-10, what is your level of pain? | user input |
| Pain Type: | user input |
| Since the time your pain or problem began, has it: | user input |
| How has this problem affected your lifestyle or ability to work? | user input |
| Have you visited a podiatrist before? | user input |
| Name of the podiatrist | user input |
| Last appointment date | user input |
| Are you a diabetic? | No |
| What athletic activities do you participate in and how often? | user input |
| Do you get leg cramps after activity? | No |
| Does foot pain limit your desired activities? | user input |
| Do you have any difficult walking? | user input |
| Any pain in the calves or buttocks when walking? | user input |
| Which of these foot problems do you have or had in the past? | Corns/Calluses,Fungal Toenails |
| Are you currently experiencing any of the following symptoms? | Fever,Muscle aches |
| Are you currently in good health? | Yes |
| Are you under the care of a physician? | No |
| Have you or any family member had or currently have any of these medical conditions: | High Blood Pressure,Diabetes |
| Have you had any serious illness/operation/ or been hospitalized? | No |
| Are you currently taking any medications? | No |
| Upload prescriptions | user input |
| Do you have any allergies? | user input |
| List any allergies you may have | user input |
| Do you use, or have you in the past, used any of the following products: | Tobacco,Alcohol |
| Smoking Status | Never smoked |
| Alcohol Intake | None |
| Are you or could you be pregnant/nursing? | No |
- Pre-populate patient details from your booking system to reduce errors
- Send an email invitation with a secure link for patients to complete their intake
- Allow patients to save their progress and complete their form at a later time
- Set up an email template and send invitation emails to multiple patients with ease
- Send an email to the patients with a copy of their response when they submit the form
Track patient responses in Google Sheets
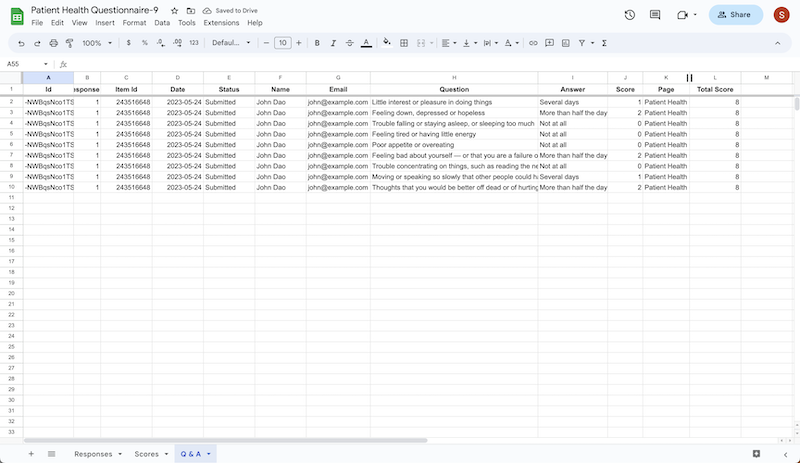
- Export patient responses to Google Sheets for easy record-keeping
- Create a custom workflow and manage your patient intake efficiently
- Use pre-built reports to easily keep track of patient progress over time
- Receive a copy of the response by email when a patient submits the intake form
- Use data in Google Sheets to integrate with EHR systems for seamless data transfer
HIPAA compliance
| Patient ID: | ****** |
| Patient Name: | ****** |
| Patient Email: | ****** |
| Patient Phone Number: | ****** |
| Marital Status: | user input |
| Date of birth: | 11/30/1899 |
| Address: | user input |
| Emergency Contact Name: | user input |
| Emergency Contact Phone: | user input |
| Relationship: | user input |
| Primary Doctor: | user input |
| Location: | user input |
| Date of service: | 11/30/1899 |
| Primary Insured (subscriber) : | user input |
| Relationship to Patient: | user input |
| Date of Birth: | 11/30/1899 |
| Phone number: | user input |
| Subscriber Employer or Plan Sponsor: | user input |
| Insurance Company: | user input |
| Subscriber ID#: | user input |
| Secondary Policy Holder Name: | user input |
| Date of Birth: | 11/30/1899 |
| Subscriber Employer or Plan Sponsor: | 11/30/1899 |
| Phone number: | user input |
| Insurance Company: | 11/30/1899 |
| What are the medical issues concerning your foot, ankle and legs?: | user input |
| Result of accident or work injury?: | No |
| On a scale of 1-10, what is your level of pain?: | 0 |
| Pain Type:: | user input |
| Since the time your pain or problem began, has it:: | user input |
| How has this problem affected your lifestyle or ability to work?: | user input |
| Have you visited a podiatrist before?: | user input |
| Name of the podiatrist: | user input |
| Last appointment date: | 11/30/1899 |
| Are you a diabetic?: | No |
| What athletic activities do you participate in and how often?: | user input |
| Do you get leg cramps after activity?: | No |
| Does foot pain limit your desired activities?: | user input |
| Do you have any difficult walking?: | user input |
| Any pain in the calves or buttocks when walking?: | user input |
| Which of these foot problems do you have or had in the past?: | Corns/Calluses, Fungal Toenails |
| Are you currently experiencing any of the following symptoms?: | Fever, Muscle aches |
| Are you currently in good health?: | Yes |
| Are you under the care of a physician?: | No |
| Have you or any family member had or currently have any of these medical conditions:: | High Blood Pressure, Diabetes |
| Have you had any serious illness/operation/ or been hospitalized?: | No |
| Are you currently taking any medications?: | No |
| Upload prescriptions: | user input |
| Do you have any allergies? : | user input |
| List any allergies you may have: | user input |
| Do you use, or have you in the past, used any of the following products:: | Tobacco, Alcohol |
| Smoking Status: | Never smoked |
| Alcohol Intake: | None |
| Are you or could you be pregnant/nursing?: | No |
- Create a HIPAA compliant intake form to safely collect, store and access patient responses
- Mark fields as Protected Health Information to secure sensitive data and limit access to PHI
- Mask PHI fields when exporting form responses to Google Sheets and sending them on email
- Pre-populate patient details in intake forms by creating secure prefill links without exposing PHI
- Limit access to patient data only for authorized personnel and minimize risk of data breaches
These reviews are reproduced without modification from Google Workspace Marketplace.
April 5, 2026
I decided to use Formesign to help me leverage HIPAA-compliant forms for my practice website. What attracted me to use them was the design/flow of the product and the price point. I had done a good bit of research on what was out there, and as someone with a small business, I wanted to get the best bang for my buck. So far, I have been incredibly pleased with the product and how I have been able to integrate my forms into my website. Customer support and setup has been great. I have zero complaints at this time and would absolutely recommend going with Formesign if you may be in a similar situation to my own (small private practice in need of HIPAA compliant forms with a pleasing interface).
— Griffin Chapple
April 22, 2026
We chose Formesign to create and collect information for incoming requests for our services. We needed to capture details of client requests and get their signatures to communicate further and provide support. The product is very adaptable, but requires a fair amount of support for a client like me who isn't tech savvy. Vipin has been extremely helpful in getting us more knowledgeable with this product. We're still learning, and appreciate the tech support we continue to receive.
— Karen Newberry
March 17, 2026
We are currently using Formesign for a non-profit academic research project on Chinese language teaching at the University of Queensland. We chose Formesign because it integrates smoothly with Google Forms and makes it easy to manage consent forms and research documentation within the same workflow. The features we found most valuable are the simple e-signature process, seamless Google Workspace integration, and ease of use for participants. This has made it much easier for us to collect and manage signed documents during our questionnaire survey process. So far our experience with the add-on has been very positive. It is straightforward to set up, reliable, and works well within the Google ecosystem, which is essential for academic research teams that rely heavily on Google tools. Overall, Formesign has been a practical and efficient solution for our research data collection process.
— Yao Li
February 25, 2026
Formesign Formesign had a truly transformative impact on my operations. The forms, signature process, and overall system they delivered are flawless. Everything works together intuitively, creating a level of efficiency and professionalism that has significantly elevated my business operations. Beyond the technical excellence of their work, what truly sets them apart is their commitment to customer service. Their one-on-one support was exceptional—courteous, responsive, and consistently focused on understanding and meeting my specific business needs. Vipin was my contact person. He was always available, patient, and thorough, ensuring that every detail was perfectly coordinated. I highly recommend Formesign to any organization looking to improve efficiency, accuracy, and workflow through customized systems. Their expertise, combined with their dedication to client satisfaction, makes them an outstanding partner.
— Mike Balducci
March 6, 2026
This product is exactly what we were looking for. It builds on a familiar tool (Google Forms), integrates seamlessly with the Google products, and adds much needs features for managing signed documents. We had tried using Adobe Acrobat forms tool and found it to be really lacking in features, especially the need for readable responsive design for mobile devices. While there is a learning curve, it is well worth it, and the personalized, live support is exceptional in an age where you normally have to play 20 questions with a chatbot. I worked with Vipin via Google Meet and screen sharing, and he was exceptionally helpful and patient and even provided additional tips on improving the appearance of the form I had designed. Bottom line - very pleased!
— Monty Morée
May 4, 2026
We are using Formesign for two of our signature workflows. We had assistance throughout the implementation process that surpassed our expectations. Formesign signature workflow now makes sure we get employee performance reviews and warning documentation forms signed by team member and their manager and allows for a supervisor approval along the way.
— Matt West
November 1, 2025
I chose Formesign because I needed a solution to link forms with signature capabilities. We are in the home service business and have a very large fleet of field operators. Formesign ability to link forms and gather signatures has removed the intense manual collection of this process out of our operation. Specifically, Vipin on the support side of Formesign has been valuable in advising on flow and making sure the process is lean. Formesign is...plug and play. Thank you!
— Jason Crossen
May 30, 2025
Besides the fact that one gets billed $216 monthly, Support took a long time to try and get things to work. Trying to get things signed on a form was such an issue and through out formatting. Way over priced, support that you have to wait till the next day to get one thing sorted and not sorted, back and forth the whole time. Frustrating customers and damage to business. I will not reccommend this company to anyone. Try JotForms so much better, and you can do much more for a fraction of the cost per year not per month.
— Francois Ohsiek
September 11, 2025
The platform is good but promises one week of premium usage based on which I chose it. Once my form was sent out to participants, it capped the responses at 24 and I was forced to pay 36 USD to keep the form active. Really disappointed by the lack of clarity and the overly tight response numbers for each tier of the plan considering how nice the platform could be.
— Nishka Khendry
July 23, 2023
I am not tech savvy. I chose formesign to help create registration links for clients. Vipid has been great in assisting me. He goes above and beyond. My company now has moved from the stone age to modern age through the ability to use this feature. Of the many features I am impressed with, the ability to update a form without needing to regenerate a link is amazing. I often make mistakes and that ability allows me to fix mistakes without needing to change everything. Thank you!!!
— Sol Evans